Having a reliable connection between a surgically implanted catheter and an external device is as critical in laboratory animal research just as it is in human medicine, particularly if you would like to access the catheter for several days, weeks or even months. The human world has standardized on luer fittings for IV connections, but luers are quite large to be used with rats and mice, both in terms of overall dimensions and dead volumes. A simple friction fit of a flexible tube over a rigid tube is still the most common connection in laboratory animal research; it is inexpensive and if done right can be reliable.
However, fear about the reliability of this connection is justified. If a catheter connection is subcutaneous, as it is with our rat and mouse Vascular Access Buttons™ (subcutaneous catheters are ideal for long-term patency), a disconnection usually means that the animal is lost. This fear leads some of our customers to have us bond the catheter to the button, a simple manufacturing step that ensures a permanent connection, but one that comes with side effects: the surgery must be done backwards, potentially exposing the catheter tip to contamination when it is tunneled through the body; a bonded round-tip catheter can’t be trimmed during surgery so must be ordered at exactly the right length for the procedure and animal size; and it means custom instead of standard parts which can impact lead times.
In this post we will summarize benchtop testing that we have done in an effort to characterize the factors that affect the reliability of an interference fit tubing connection.
Testing of Catheter Disconnection Forces
We measured the force required both to pull a 10cm length of flexible tubing off of a rigid connector, and also the force down on the plunger of a 1cc BD syringe required to blow an occluded 10cm segment of tubing off the connector. We have focused on 3Fr / 22ga connections that are commonly used with catheterized rats. The tubing was primed, submersed in 35-39°C water and given time to warm up to simulate subcutaneous conditions. New tubing was used for each test. We looked at the following factors:
- Tubing material
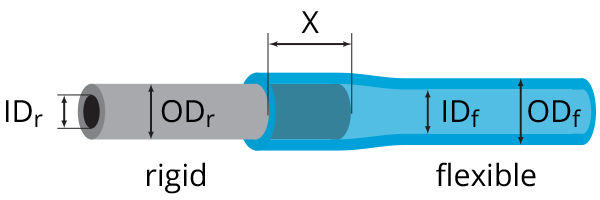
- Overlap (X)
- Stretch (ODr-IDf)
- Rigid tubing features
- Flexible tubing features
Tubing material

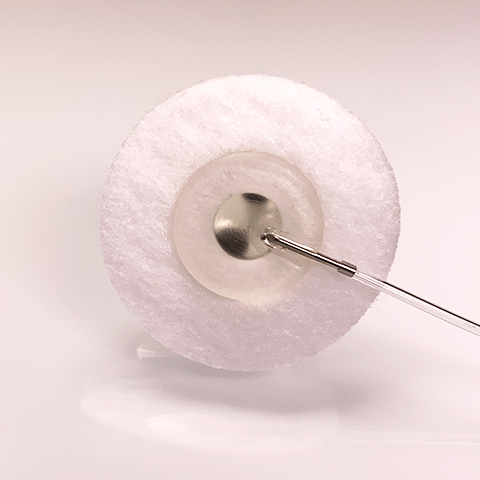
3Fr PU on 22g connector of VAB with 3mm overlap
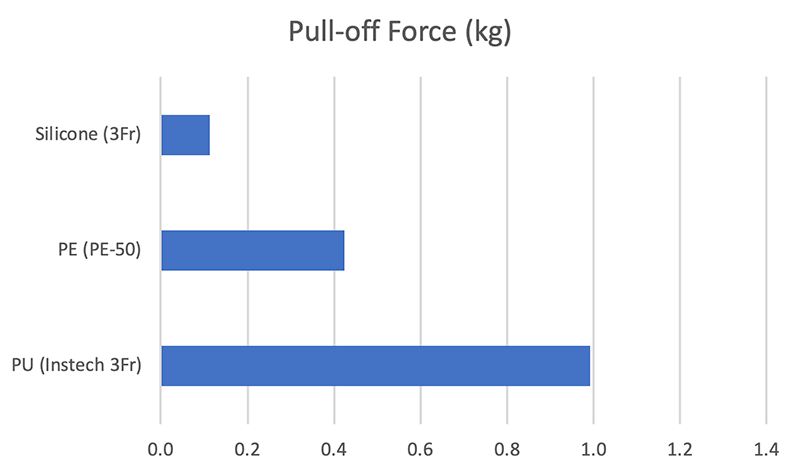
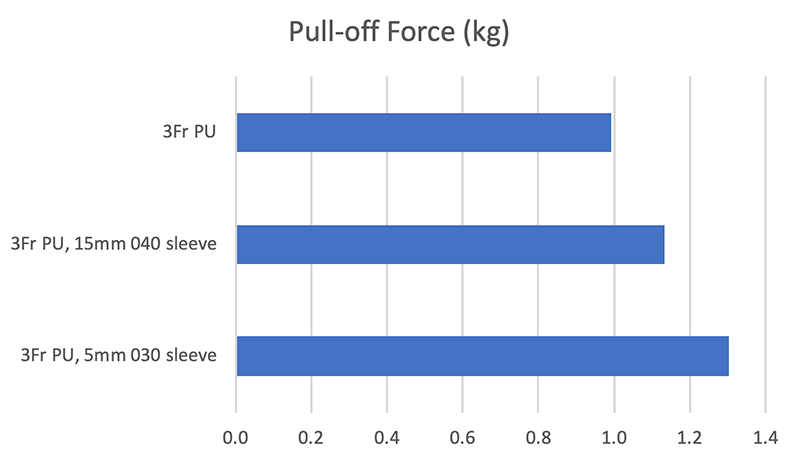
Pull-off force. Polyurethane (PU) tubing is significantly more difficult to pull off the connector than is silicone or polyethylene (PE) tubing, requiring 1kg of force, which is hard to imagine happening in a 300gm rat. At the point of disconnection the 10cm PU tubing segment is stretched four times its original length, while silicone and PE stretch 50% or less before disconnecting.
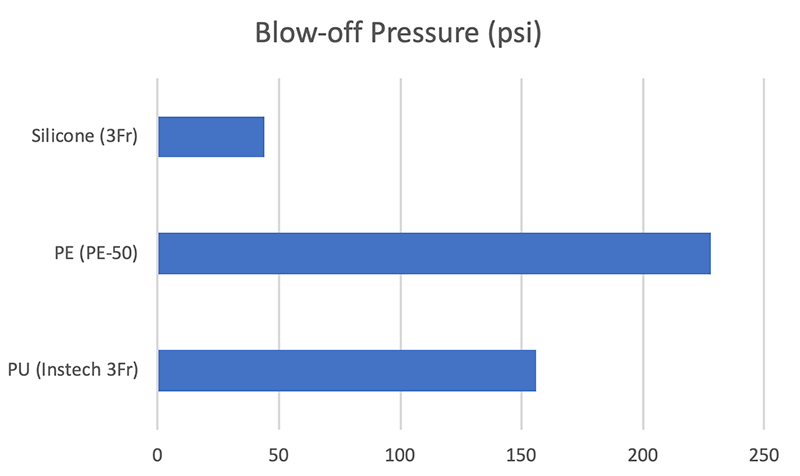
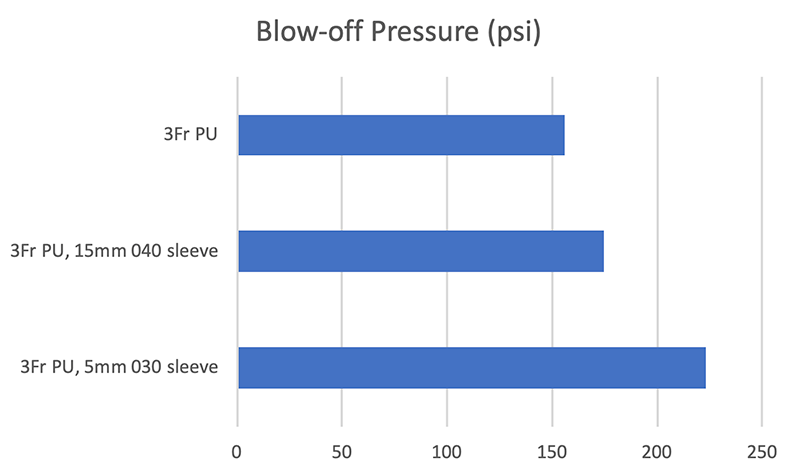
Blow-off pressure. You can generate a tremendous amount of pressure with a syringe: 3lbs of force with your thumb on the plunger of a 1cc syringe will generate over 100psi of pressure inside a catheter if it is fully occluded. (For comparison, a mountain bike tire is typically inflated to 30psi.) These pressures have no place inside a living animal. At around 100psi a slip-fit luer placed with a normal amount of force onto a Becton-Dickinson 1cc syringe will separate from the syringe. To conduct these tests we had to jam the injector luer on the syringe (see video). Only the silicone tube blows off with less than 100psi. Polyurethane, the standard catheter material, blows off at approximately 150psi while stiff polyethylene blows off at 225psi.
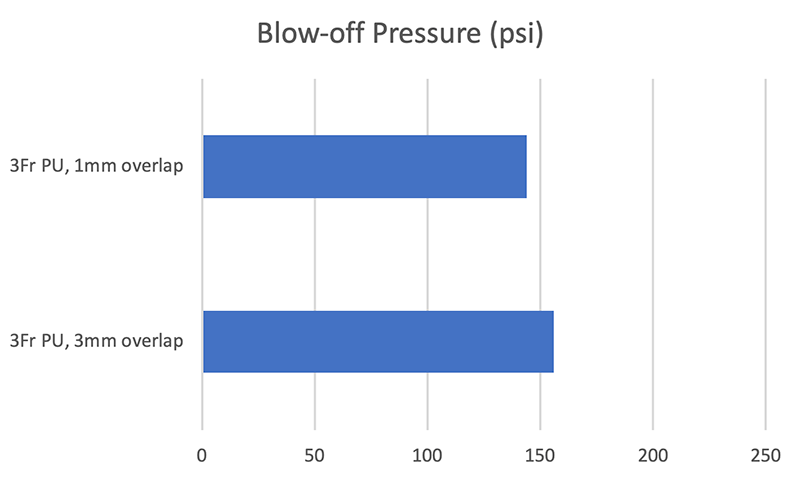
Overlap (X)
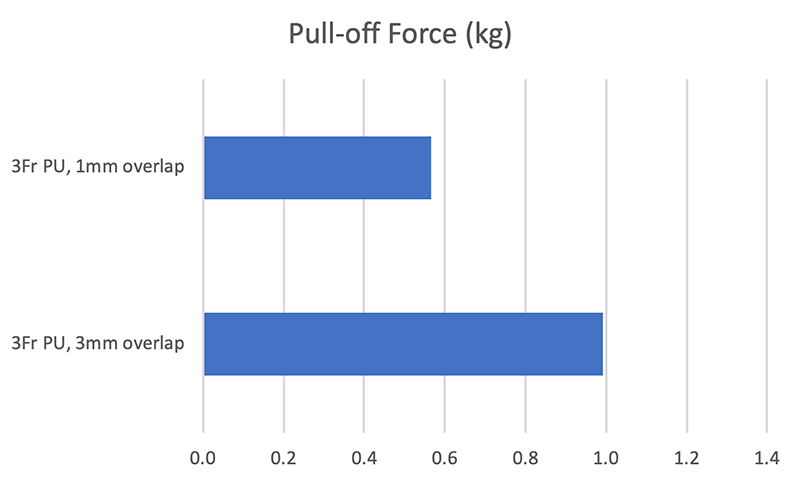
3Fr PU on 22g connector of VAB with 1mm overlap
Taking the time in surgery to push the catheter fully onto the connector will help prevent a disconnection. When the same 3Fr PU catheter is placed on a 22ga connector with only 1mm of overlap instead of 3mm, the pull-off force drops 40%, from 1.0kg to 0.6kg. The blow-off pressure drops only slightly and remains well over 100psi, a level which trained technicians should never reach.
Stretch (ODr-IDf)
The ideal amount of stretch of a flexible tube over a rigid tube depends on the flexible tube material. For 3Fr polyurethane over 22ga we have found that a .003-.004in (.08-.10mm) interference fit is a good compromise between pull-off resistance and ease of connection. If the tubing inner diameter is too small it can be difficult to get a good overlap (X) and so the benefit of the tighter fit will be lost.
[summary of testing data with graphs to come in a future update]
A tight tolerance on the inner diameter of flexible tubing is a challenge for tubing extruders but is important for a consistently good connection. (The outer diameter of stainless steel hypodermic tubing rarely varies significantly.) If tubing from two manufacturers have the same nominal ID but one manufacturer can hold ±0.001in while another can only hold ±0.002in, that can mean a meaningful difference in pull-off force. If you are a surgeon and notice that some catheters are sliding on the connectors easily while others from the same batch are more difficult, you should be concerned and contact your catheter manufacturer.
Rigid Tubing Features
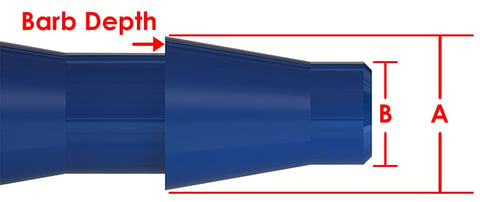
Barb dimensions (image courtesy of ISM: Barb Connectors in Depth - Design and Function)
Barb fittings are often used for industrial hose connections and are sometimes mentioned as a potential improvement to rodent catheter connections; they are found on some subcutaneous Vascular Access Ports used with large animals (including humans). Disadvantages of barbs are a high manufacturing cost for parts with consistent dimensions, and a potentially sharp point which could puncture the catheter.
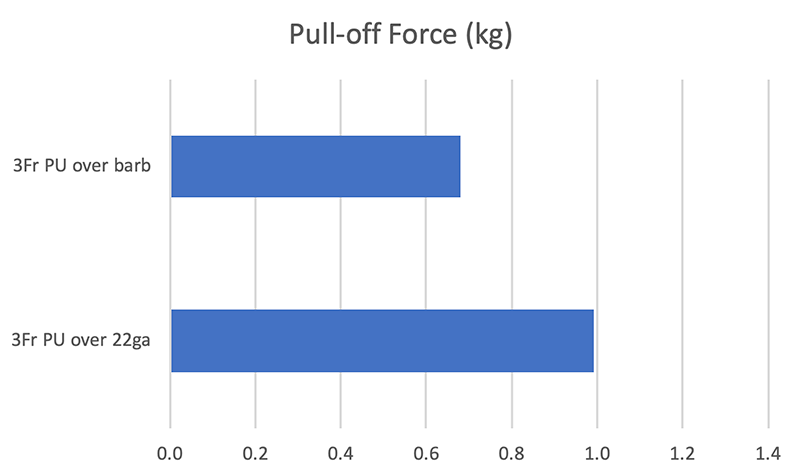
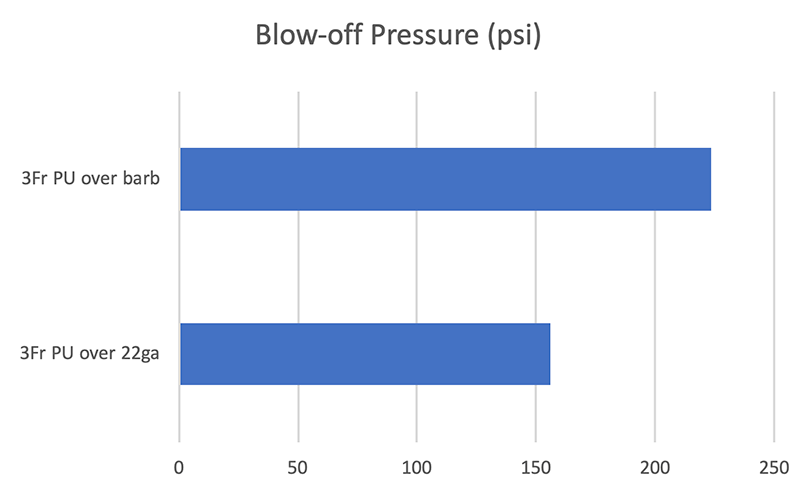
We manufactured a barb with A of .79mm and depth of .08mm and compared it to straight 22ga tubing (OD of 0.71mm). Surprisingly the pull-off force of 3Fr PU from the barb was 30% lower than from the straight tubing. The barb fitting held until approximately 225psi of blow-off pressure compared to 150psi for the straight tubing, both well above the 100psi level at which a typical slip-fit luer will separate.
Flexible Tubing Features
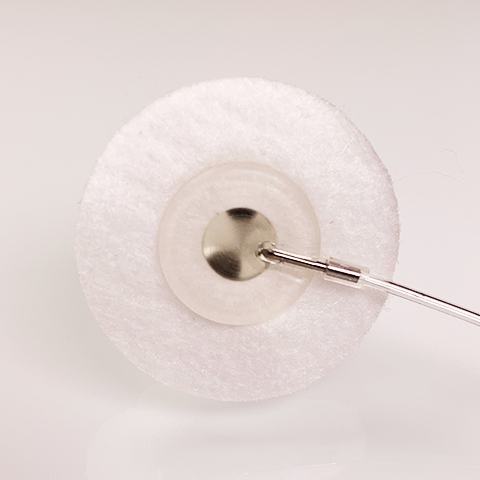
3Fr PU on 22g connector of VAB with 5mm sleeve
Sleeves which are slid over the tubing connection during surgery are a simple addition to a pre-made catheter and provide some extra pull-off and blow-off resistance.
We tested a 15mm silicone sleeve with an ID that matches the OD of the 3Fr PU tubing and then a 5mm silicone sleeve with a 0.010in (0.25mm) interference fit over the PU. Both helped. The looser sleeve increased pull-off resistance by 14%, the tighter one by 31%. The looser sleeve improved blow-off resistance by approximately 12%, the tighter one by 43%.
Conclusions
A simple slip fit of a 3Fr polyurethane catheter over a 22ga connector should provide a reliable long-term subcutaneous connection if the inner diameter of the catheter is between .61 and .63mm and it is placed on with at least 3mm of overlap. Sliding a sleeve over the joint will give some added protection against disconnections.
Silicone and polyethylene catheters should be avoided. Barb fittings do not seem to help; it is significantly easier to pull a 3Fr PU catheter off of the single barb described here than it is a straight 22ga tube.
Blowing a properly fitted catheter off a connector is possible but requires tremendously high pressures, over 100psi, which should never be applied to a living animal. Technicians should be able to feel the excessive force even with small syringes, and if they are not sure it should be part of their training. Luer locks should not be needed in laboratory animal research, as the failure of a slip fit luer (at about 100psi for high-quality syringes, lower for cheaper models) is a sure sign that pressures are excessive.
Syringe pumps, on the other hand, will not stop pushing unless they have an occlusion alarm. Even the entry-level Harvard pump will generate 16kg of linear force before it stalls, translating into 1300psi with a 1cc syringe. If you are using a pump without a sensitive occlusion alarm, you and your IACUC should be prepared to accept some level of infusion set failures and loss of animals.
If you have experienced disconnections we hope these measurements will help guide you to the root cause. Perhaps your catheter inner diameter is varying too much, or your surgeon was rushed and did not slide it over the connector far enough. Check to see if there is a step in your procedures where excessive pressures could be created. Or more likely it is a combination of factors.
Additional testing is needed to characterize other connection dimensions (such as 2Fr to 25ga which is common for mouse catheters), and the impact of lubricious lock solutions such as glycerol. If you have other factors that you would like us to investigate, please contact us.
Appendix
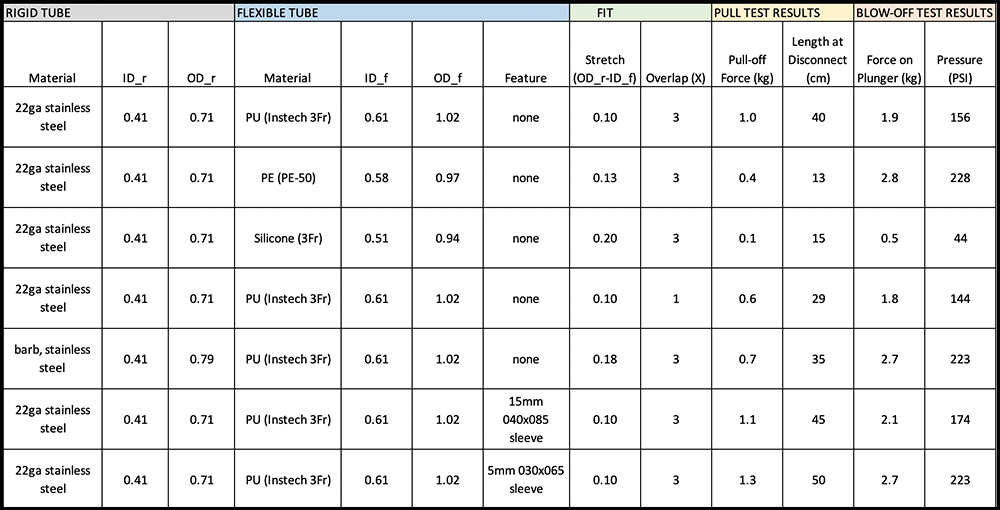
Test Data (dimensions in mm unless otherwise noted)